Classification of Membranoproliferative Glomerulonephritis According to New Evolving Classification System by Using Immunofluorescence Technique
*Rahman DA,1 Asaduzzaman,2 Saleheen S,3 Sultana S,4 Banu SG 5
Abstract
Background: Membranoproliferative glomerulonephritis (MPGN) are progressive diseases with poor prognoses. Recently, a newly proposed classification of these diseases separated them into immune complex – and complement- mediated diseases. We investigated the frequency of C3 glomerulopathy among histologically diagnosed MPGN patients by using immunofluorescence study.
Methods: We conducted a cross sectional study was carried out at the Department of Pathology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka during the period from June 2015 to December 2016. The histopathological, immunofluorescence studies were carried out at the Department of Pathology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka.
Results: We found 8 cases of complement mediated MPGN (C3 glomerulopathy) out of 67 cases of MPGN, accounting for 12% of the total cases of MPGN. Histomorphological and other clinical parameters in immune complex mediated MPGN and complement mediated MPGN show no significant difference.
Conclusion: Complement-mediated glomerulonepathy was present in 12% of patients previously diagnosed with MPGN.
[Journal of Histopathology and Cytopathology, 2019 Jul; 3 (2):76-85]
Keywords: Membranoproliferative glomerulonephritis, C3 glomerulopathy, Immunofluorescence
- *Dr. DM Arifur Rahman, Assistant Professor, Pathology, TMSS Medical College, Bogura. arifurrahmandm@gmail.com
- Asaduzzaman, Lecturer, Pathology, Sheikh Sayera Khatun Medical College, Gopalgonj
- Saied Saleheen, Assistant Professor (Current Charge), Pathology, Sheikh Hasina Medical College, Tangail.
- Sabera Sultana, Lecturer, Virology, Rajshahi Medical College
- Sultana Gulshana Banu, Associate Professor, Pathology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka.
*For correspondence
Introduction
Membranoproliferative glomerulonephritis (MPGN) is the fourth most common cause of primary glomerulonephritis in Bangladeshi patients and seventh most common cause of primary glomerulonephritis in Indian patients.1,2 Because the proliferation is predominantly in the mesangium but may also involve the capillary loops, membranoproliferative glomerulonephritis is also known as mesangiocapillary glomerulonephritis.3 MPGN accounts for 10% to 20% of cases of nephrotic syndrome in children and young adults.4
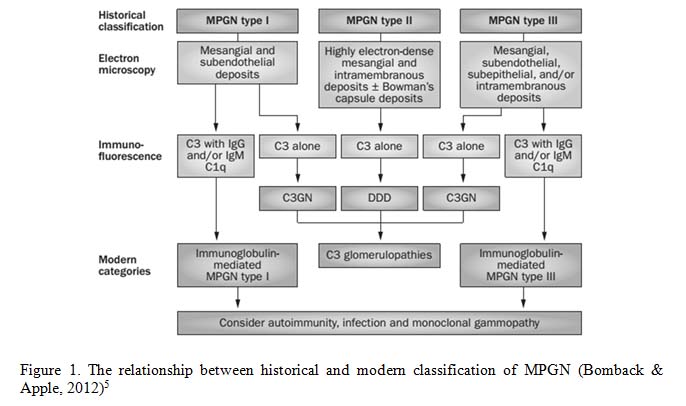
Traditionally, primary MPGN has been classified based on the findings of electron microscopy (EM) as MPGN type I (MPGN I), MPGN II and MPGN III. This classification does not reflect the disease pathogenesis. It is proposed that MPGN be classified into two major groups on the basis of Immunofluorescence (IF) findings: immunoglobulin (Ig)-mediated and complement-mediated (C3G) membranoproliferative glomerulonephritis(MPGN). If the IF studies show predominantly C3 and are negative or show no significant staining for Igs, this is called complement mediated MPGN, also known as C3 glomerulopathy. If immunoglobulins are present on IF studies, it is considered as Ig mediated MPGN.5-8
C3 glomerulopathy again classified as dense deposit disease (DDD) (formerly membranoproliferative GN type II and C3 glomerulonephritis (C3GN) based on electron microscopic findings. C3 glomerulopathies in which the deposits do not fulfill the criteria for dense deposit disease have been designated as ‘C3 glomerulonephritis’.9
The term C3 glomerulonephritis was coined to describe glomerular lesions in which there is glomerular accumulation of C3 with little or no immunoglobulin in the absence of the characteristic highly electron-dense transformation seen in dense deposit disease. Practically according to the concensus meeting towards the definition of C3 glomerulopathy stated that C3 glomerulopathy should be used as a morphological termfor those cases with dominant staining for C3. Dominant is defined as C3 intensity ≥2 orders of magnitude more than any other immune reactant on a scale of 0 to 3 (including 0, trace, 1+, 2+, 3+).7
The new classification system based on immunofluorescence findings has been proposed to replace the traditional classification system in order to better identify the underlying causes of MPGN and to provide guidance for more individualized treatment. Eculizumab, the first available anticomplement therapy, blocks at the level of complement (C5) and has revolutionized the treatment of complement-mediated diseases as well as C3 glomerulopathy.5

Objectives
The main objective of the present study is to find out the distribution of complement mediated membranoproliferative glomerulopathy in Bangladesh. A second objective is to study the various histopathological changes and immunofluorescence pattern in renal biopsy specimens with MPGN as well as to compare between various clinical presentation and biochemical parameters between immune complex mediated MPGN and complement mediated MPGN.
Methods
This cross sectional study enrolled 67 cases of membranoproliferative glomerulonephritis during the period from June 2015 to December 2016. Histopathological and immunofluorescence studies were carried out at the Department of Pathology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka. Cases diagnosed as membranoproliferative glomerulonephritis, based on renal biopsy findings; irrespective of age and sex were included in this study. Cases diagnosed as lupus nephritis, post streptococcal glomerulonephritis, IgA nephropathy and C1q nephropathy were excluded from the study.
All clinical information were recorded in a pre-designed proforma before doing histopathology and direct immunofluorescence microscopy including patient’s age, sex, clinical presentation and results of laboratory investigation like urinary total protein (UTP), urinary RBCs, serum creatinine, blood urea, anti-nuclear antibody (ANA), anti-double stranded DNA (Anti-ds DNA) antibody etc.
Two samples of renal tissue were obtained from each case. Specimen for light microscopy was preserved in 10% formalin and that for immunofluorescence in normal saline. After arrival at the pathology department, tissue in 10% formalin was embedded in paraffin block and processed routinely. Then sections were cut thin (3-4 µm) with microtome and stained with haematoxyllin and eosin, periodic acid Schiff (PAS) and methenamine silver stains. The tissue in normal saline was stored at -20oC temperature in deep freeze for subsequent cryostat sectioning. The sections were stained by fluorescein isothiocyanate (FITC) tagged conjugated rabbit polyclonal anti human IgG, IgA, IgM, complement component 3 (C3), fibrinogen and complement component 1q (C1q).
Results
Among 67 biopsies, 59 cases (88%) were diagnosed as immune complex mediated MPGN. Eight (12%) cases were found to be conforming to complement mediated MPGN (C3 glomerulopathy), as defined by the diagnostic criteria mentioned earlier.
The mean age of patients with immune complex mediated MPGN was 35.71±11.76 and with complement mediated MPGN was 35.87±14.98. The mean age difference is not statistically significant (p>0.05) between two groups. In cases of immune complex mediated MPGN, number of male patients were 31 (53%) and female patients were 28 (47%). In cases of complement mediated MPGN, number of male patient was 5(62%) and female patient was 3(38%).
Nephritic syndrome was the most common presentation in cases of complement mediated MPGN (50%) compared to immune complex mediated MPGN (27%). On the other hand nephrotic syndrome was the most common presentation (58%) in cases of immune complex mediated MPGN compared to complement mediated MPGN (37.5%).
The mean creatinine value of immune complex mediated glomerulonephritis was 1.56 mg/dl and of complement mediated glomerulonephritis was 1.33 mg/dl. Serum C3 level decreased in 62% and 57% cases of immune complex mediated and complement mediated glomerulonephritis respectively. This differences are not statistically significant between two groups (p>0.05).
Crescent formation is observed 2 cases (3%) of immune complex mediated MPGN and one case of complement mediated MPGN (12.5%). Haematuria was present in 69% cases of immune complex mediated MPGN. On the other hand haematuria was present in 75% cases of complement mediated MPGN. These differences are not statistically significant (P value is >0.05)
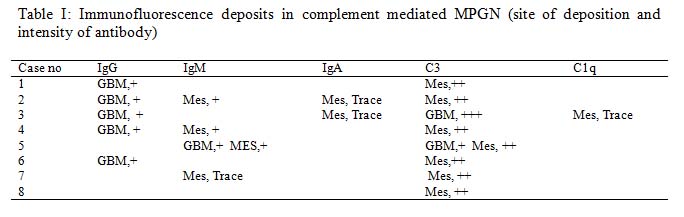
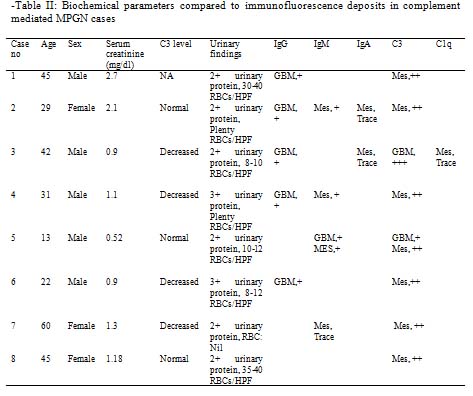
Table I shows immunofluorescence deposits in complement mediated MPGN. It describes sites of deposition of antibody and staining intensity. Staining intensity is expressed by a scale of 0 to 3 including 0, trace, 1+, 2+, 3+ (Pickering et al., 2013). Table II shows biochemical parameters compared to immunofluorescence deposits in complement mediated MPGN cases.
Discussion
The traditional classification of membranoproliferative glomerulonephritis is confusing. It is not based on disease pathogenesis and the types are overlapping. A new classification system of membranoproliferative glomerulonephritis based on immunofluorescence finding has been proposed. It helps to identify the underlying causes of MPGN and to provide guidance for more individualized treatment. This is a cross sectional study carried out to find out the distribution of immunoglobulin mediated and complement mediated membranoproliferative glomerulonephritis as well as to detect immunofluorescence deposits in renal biopsy specimens with MPGN. Clinical presentations and biochemical parameters in immune complex mediated MPGN and complement mediated MPGN were also observed.
A total of 67 membranoproliferative glomerulonephritis cases were included in this study. Clinical information and written consent were taken from the patients or their attendants. All clinical information were recorded in a pre-designed proforma. Routine H&E, PAS and methenamine silver stained sections of the renal biopsy samples were examined by two experienced pathologists. Sections were examined for changes in four components: glomeruli, tubules, interstitium and blood vessels. Cryostat sections were examined under fluorescence microscope for antibody deposition in the renal tissue. We categorized 59 cases (88%) as immune complex mediated MPGN and 8 cases (12%) as complement mediated MPGN out of 67 cases. Similar studies were conducted by Lu et al., in 2012, in China, Woo et al., in 2014, in South Korea, Pavinic and Miglinas, in 2015, in Lithuania and Mathur et al., in 2015, in India. They showed the percentage of C3 glomerulopathyin a series of studies on previously diagnosed MPGN cases as 20%, 4.3%, 8.6% and 1.16%, respectively.10-13
The mean age of immune complex mediated MPGN cases was 35.71 years and of complement mediated MPGN (C3 glomerulopathy) cases was 35.87 years. Study conducted by Servais et al had showed the mean age of presentation of their C3 glomerulonephritis cases 30.3 years (SD±19.3).9 We had 5 cases of pediatricpatients (7.5% of total) out of which 4 were immune complex mediated MPGN (80%) and 1 was C3 glomerulopathy (20%).9 This finding is comparable with the study conducted by Giedraite et al on pediatric patients. They diagnosed 8 out of 23 pediatric MPGN cases as C3 glomerulopathy which was about 34% of total MPGN cases.14
Most of the patients of our study with both immune complex mediated and complement mediated MPGN are male. We found 53% and 62% male patients in cases of immune complex mediated MPGN and complement mediated MPGN respectively. Study conducted by Walker et al reveal no significant sex difference.15
At presentation, almost all patients had proteinurea and most of the patients had haematuria. Nephrotic syndrome was present in 57% patients of immune complex mediated MPGN and 37% patients of complement mediated MPGN. The study conducted by Servais et al showedthat 38% of patients with dense deposit disease (MPGN type II) had nephrotic syndrome at presentation as compared with 65% of patients with MPGN type I.9
Nephritic syndrome was present in 27% patients of immune complex mediated MPGN and 50% patients of complement mediated MPGN in the present study. The study conducted by Mathur et al showed 50% patients with complement mediated MPGN of their study cases had nephritic syndrome and 50% had nephrotic syndrome at presentation.13
Haematuria was present in 75% cases of complement mediated MPGN and 69% cases of immune complex mediated MPGN. The study conducted by Nasr et al had showed 87% patients of dense deposit disease had haematuria on presentation.16
Mean serum creatinine value in immune complex mediated MPGN was 1.56 mg/dl. It was slightly lower in complement mediated MPGN (1.33 mg/dl). Mean serum creatinine was 2.2 mg/dl on 32 patients diagnosed as dense deposit disease.16
Serum C3 level was decreased in 62% cases and normal in 38% cases of immune complex mediated MPGN in our study. On the other side serum C3 level was decreased in 57% cases and normal in 43% cases of complement mediated MPGN. The study conducted by Servais et al showed that 40% of the C3GN patients had low C3 levels in circulation, and 46% patients of MPGN type I showed low C3 level.9
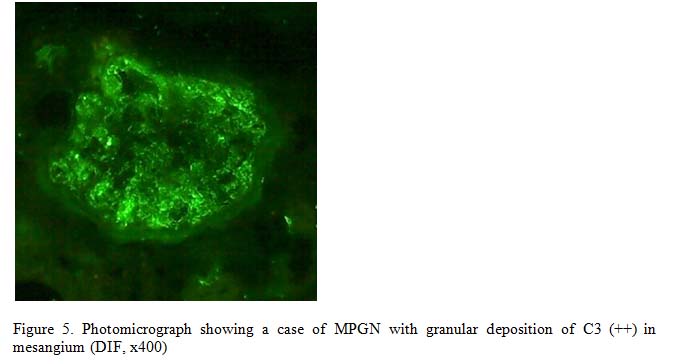
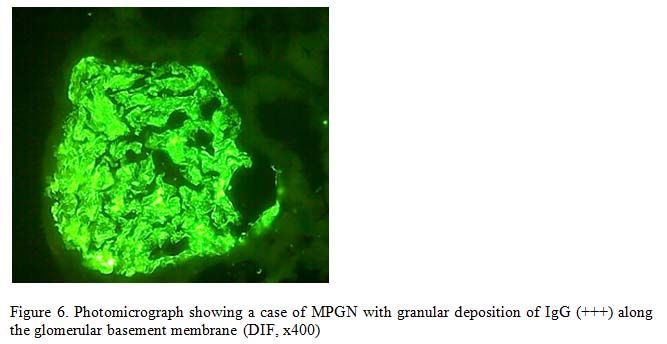
According to Concensus Report on C3 Glomerulopathy published in, C3 glomerulopathy is defined as C3 intensity ≥2 orders of magnitude more than any other immune reactant on a scale of 0 to 3 including 0, trace, 1+, 2+, 3+. In the present study immunofluorescence microscopy revealed, in most cases of complement mediated MPGN, a granular mesangial deposition of C3 with 2+ staining intensity. In cases with other immunoreactants, the dominant mesangial staining was C3 with at least two order intensity than others.7 The second most common deposited antibody was IgG along the glomerular basement membrane followed by IgM and IgA in the mesangium. We found only one case having mesangial deposition of C3 without any other antibody. Nasr et al and walker et al noted intense staining for C3 along the glomerular basement membrane and in the glomerular mesangial regions in their cases. Nasr et al also showed that immunoglobulins were absent or showed only focal and segmental staining with much less intensity than C3. They found IgM the most common second antibody; IgG and especially IgA were less common. Giedraite et al showed the second most common deposited antibodyamong 8 cases of C3 glomerulopathy was IgG followed by IgM.16
In the present study the immunofluorescence microscopy of immune complex mediated MPGN showed IgG antibody in 50 (86%) cases which was seen along glomerular basement membrane. 4 cases (6%) showed deposition of IgG in mesangium. Second most common immunoreactant was IgM followed by C3, IgA and C1q. 47 (79%) cases showed positive staining for IgM and 46 (77%) cases showed positive staining for C3. IgA positivity was seen in one third cases. Davis and Cavallo showed that in the immune complex variant of MPGN, the most consistent finding was positive IgG staining in granular pattern along the glomerular basement membrane.17 IgM was less common than IgG, but it was present in 86% of patients in one series, and 73% in another.18,19
Conclusion
In the present study we have classified the membranoproliferative glomerulonephritis cases according to the new classification system which is based on detection of immunoreactants in the renal tissue. The immunoreactants reflect the underlying pathogenesis of the disease process. We think this classification can help to manage the patients in a developing country like ours where modern facilities including electron microscope are lacking.
References
- Hossain MT, Begum M, Rahman AN, Kamal M. Immune deposits in glomerular diseases and their clinical, histopathological and immunopathological correlation. Bangladesh Journal of Pathology. 2011;26(1):14-9.
- Narasimhan B, Chacko B, John GT, Korula A, Kirubakaran MG, Jacob CK. Characterization of kidney lesions in Indian adults: towards a renal biopsy registry. Journal of nephrology. 2006;19(2):205-10.
- Jennette JC, Olson JL, Silva FG, DAgati VD. Heptinstalls pathology of the kidney. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2015
- Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran pathologic basis of disease, professional edition e-book. Elsevier health sciences; 2014 Aug 27.
- Bomback AS, Appel GB. Pathogenesis of the C3 glomerulopathies and reclassification of MPGN. Nature Reviews Nephrology. 2012;8(11):634.
- Sethi S, Fervenza FC. Membranoproliferative glomerulonephritis: pathogenetic heterogeneity and proposal for a new classification. In Seminars in nephrology 2011;31(4): 341-348).
- Pickering MC, D’agati VD, Nester CM, Smith RJ, Haas M, Appel GB, Alpers CE, Bajema IM, Bedrosian C, Braun M, Doyle M. C3 glomerulopathy: consensus report. Kidney international. 2013;84(6):1079-89.
- Rabasco Ruiz C, Rabasco-Ruiz C, Huerta Arroyo A, Huerta-Arroyo A, Caro Espada J, Caro-Espada J, Gutiérrez Martínez E, Gutiérrez-Martínez E, Praga Terente M, Praga-Terente M. C3 glomerulopathies. A new perspective on glomerular diseases. Nefrología (English Edition). 2013;33(2):164-70.
- Servais A, Frémeaux-Bacchi V, Lequintrec M, Salomon R, Blouin J, Knebelmann B, Grünfeld JP, Lesavre P, Noël LH, Fakhouri F. Primary glomerulonephritis with isolated C3 deposits: a new entity which shares common genetic risk factors with haemolytic uraemic syndrome. Journal of medical genetics. 2007;44(3):193-9.
- Woo SA, Ju HY, Kwon SH, Lee JH, Choi SJ, Han DC, Hwang SD, Hong SY, Jin SY, Gil HW. Reanalysis of membranoproliferative glomerulonephritis patients according to the new classification: a multicenter study. Kidney research and clinical practice. 2014;33(4):187-91.
- Lu Y, Shen P, Li X, Xu Y, Pan X, Wang W, Chen X, Zhang W, Ren H, Chen N. Re-evaluation of the classification system for membranoproliferative glomerulonephritis. In New Insights into Glomerulonephritis 2013;181:175-184).
- Pavinic J, Miglinas M. The incidence of possible causes of membranoproliferative glomerulonephritis: a single-center experience. Hippokratia. 2015;19(4):314.
- Mathur M, Sharma S, Prasad D, Garsa R, Singh AP, Kumar R, Beniwal P, Agarwal D, Malhotra V. Incidence and profile of C3 Glomerulopathy: A single center study. Indian journal of nephrology. 2015;25(1):8.
- Giedraite N, Besusparis J, Masalskiene J, Cerkauskiene R, Jankauskiene A. New Classification of Paediatric Membranoproliferative Glomerulonephritis Cases in Lithuania. Inpediatrnephrol. P–301. Abstracts-48th ESPN Meeting, Brussels 2015 Sep 1.
- Walker PD, Ferrario F, Joh K, Bonsib SM. Dense deposit disease is not a membranoproliferative glomerulonephritis. Modern pathology. 2007;20(6):605.
- Nasr SH, Valeri AM, Appel GB, Sherwinter J, Stokes MB, Said SM, Markowitz GS, D’Agati VD. Dense deposit disease: clinicopathologic study of 32 pediatric and adult patients. Clinical Journal of the American Society of Nephrology. 2009;4(1):22-32.
- Davis BK, Cavallo T. Membranoproliferative glomerulonephritis. Localization of early components of complement in glomerular deposits. The American journal of pathology. 1976;84(2):283.
- Zucchelli P, Sasdelli M, Cagnoli L, Donini U, Casanova S, Rovinetti C. Membranoproliferative glomerulonephritis: correlations between immunological and histological findings. Nephron. 1976;17(6):449-60.
- Morel-Maroger L, Leathem A, Richet G. Glomerular abnormalities in nonsystemic diseases: Relationship between findings by light microscopy and immunofluorescence in 433 renal biopsy specimens. The American journal of medicine. 1972;53(2):170-84.