![]()
Comparing PAP Smear Cytology with High Risk Human Papilloma Virus DNA Test in Patients of Cervical Lesions
*Ansari NP,1 Rahman AN,2 Saleh AM,3 Shahida SM4
Abstract
Cervical cancer is the second most frequent type of cancer worldwide. More than eighty eight percent deaths from cervical cancer occur in developing countries. In developed countries, the cases and deaths have declined markedly due to their extensive screening programs. The present study was undertaken to assess precancerous and cancerous cervical lesions by cytology as well as Human Papilloma virus (HPV) DNA identification and their comparison with histopathology in Visual Inspection of Cervix with Acetic Acid (VIA) positive cases. This observational study was carried out at the Department of Pathology in collaboration with the Department of Gynaecology and Obstetrics of Mymensingh Medical College Hospital and Department of Microbiology and Hygiene of Bangladesh Agriculture University for HPV DNA detection during the period of July 2012 to June 2013. Study was carried out among 160 VIA positive patients and selected by non-random judgment sampling from the colposcopy clinic. Out of 160 cases, only 40(25.00%) were found HPV DNA positive, while the rest 120(75.00%) cases were negative. Among positive cases 77.50% were cancerous cases and 22.50% were precancerous cases. It was further revealed that in cancerous cases, 86.11% were HPV DNA positive. PCR showed low sensitivity, probably due to sampling error and inclusion of all cases (chronic cervicitis, precancerous and cancerous lesion). The statistical value of accuracy, sensitivity and specificity of Pap smear cytology, HPV DNA test and histopathology yielded some important directives. The sensitivity values of Pap smear cytology and HPV DNA were found 87.50% and 88.89% respectively. Thus Pap smear test showed almost equal sensitivity to DNA test. The accuracy of the Pap smears and HPV DNA in this study was 88.13% and 96.88% respectively. The accuracy of Pap smears is lower than HPV DNA tests. The present study showed the significant relationship between cytological with HPV DNA test and histopathological diagnosis. But cytology and HPV DNA testing are not suitable as a single test. In conclusion, it can be stated that combination cytology (Pap smear), histopathology and new technologies such as HPV DNA typing would ultimately be more useful.
[Journal of Histopathology and Cytopathology, 2017 Jul; 1 (2):102-109]
Key words: Pap smear cytology, Human Papilloma virus, Cervical lesions
- *Dr. Nazma Parvin Ansari, Assistant Professor of Pathology, Community Based Medical College, Mymensingh. palashansaripath@gmail.com
- AJE Nahar Rahman, Honorary Professor, Department of Pathology, BIRDEM, Dhaka.
- AFM Saleh, Professor of Pathology, Mymensingh Medical College, Mymensingh.
- S M Shahida, Assistant Professor of Gynae & Obs, Dhaka Medical College, Dhaka
*For correspondence
Introduction
Cervical cancer is the second most frequent type of cancer and the leading cause of mortality among women worldwide.1 According to WHO/ICO Report2 the incidence rates of cervical cancer in Bangladesh are highest compared to other countries of South Asia and the annual mortality is 11.6 per 1,00,000 women. The report further stated that 50.19 million women are at risk of developing cancer. Each year 17,686 women are diagnosed with cervical cancer and 10,364 die from the disease. It is observed that the cases and deaths have declined markedly in developed countries from approximately 1.4 to 1.7 per 1,00,000 women and this reduction was mainly as a result of extensive screening programs.3,4
There is worldwide agreement that screening test for cervical cancer is a necessity because it separates healthy persons from those with a high probability of having the disease. The lower incidence in developed countries is due to the access of women to screening test, which allows precancerous lesions to be detected and treated before they develop into full blown cancer.5 Popular screening tests are Papanicolaou (PAP) smear, visual inspection of cervix with acetic acid (VIA) and HPV DNA test. The uptake of screening test in many developing countries is still poor.6,7,8,9 VIA has been introduced by the Government of Bangladesh to screen mass population because it is easy procedure and cost effective. All the government medical college hospitals, district hospitals, maternal and child welfare centers and some of the urban primary health care centers have facilities for VIA test free of cost by the support of UNFPA Bangladesh. Bangabandhu Sheikh Mujib Medical University (BSMMU) is collaborating with Government of Bangladesh in expansion of these facilities.10
At the present time a good deal of attention is being paid to screening for early confirmatory detection of cancer. The present study was undertaken to assess precancerous and cancerous cervical lesion by cytology in VIA positive cases and the relationship between the high risk Human Papilloma viruses.
Methods
This was a descriptive, cross-sectional type of observational study. The study was carried out in the Department of Pathology, Mymensingh Medical College. Patients of different age groups were selected from colposcopy clinic of Mymensingh Medical College Hospital. Duration of study was one year ranging from July 2012 to June 2013. A total of 160 patients were selected in the mentioned study period with follwing criteria which were (1) VIA positive married married females aged 30-60 years and (ii) who were married for at least 10 years but below 30 years of age. The study excluded patients who were pregnant, below twenty years of age and patient at menstruating period. PAP smears were collected with Ayer’s spetula and cytobrash by gynaecologists in the colposcopy clinic in the department of Mymensingh Medical College Hospital. Colposcopy guided punch biopsy were taken by same gynecologists from the suspected lesions of the VIA positive cases. Histopathological examination of the biopsy samples were done in the department of Pathology, Mymensingh Medical College. HPV DNA detection by Polymerase Chain Reaction was done from paraffin embedded tissue blocks. HPV type 16, 18, 31 and 52 primers were used.
Results
The study was undertaken to assess the precancerous and cancerous cervical lesion by cytology in VIA positive cases and compare their results with histopathology and high risk Human Papilloma Virus (hr-HPV) DNA test. Table I shows that 36 (22.50%) patients were in 20 to 29 years age group, 72 (45.00%) patients belonged to the age group 30 to 39 years, 37 (23.10%) cases in 40 to 49 years age group and 15 (9.40%) cases in 50-59 years group.
Table I: Age distribution of the subjects
| Age Groups in Year | Frequency | % |
| 20-29 | 36 | 22.5 |
| 30-39 | 72 | 45 |
| 40-49 | 37 | 23 |
| 50-59 | 15 | 9.4 |
| Total | 160 | 100 |
*Mean () = 38.00 Years; Standard Deviation (SD) = 8.15 Years.
Table II shows the results of Pap smears diagnosis. On cytological examination, 63 (39.40%) cases were diagnosed as Negative for Intraepithelial Lesion or Malignancy (NILM), followed by 5 (3.10%) cases diagnosed as lesions with Atypical Squamous Cells of Undetermined Significance (ASCUS) and other 5 (3.10%) cases were found Atypical Squamous Cell that cannot exclude HSIL (ASC- H), 40 (25.00%) patients with Low Grade Squamous Intraepithelial Lesions (LSIL); 17 (10.60%) patients with high grade squamous intraepithelial lesion (HSIL)and 30 (18.75%) patients were diagnosed as Squamous Cell carcinoma (SCC).
Table II: Cytological (Pap smear) diagnosis of cervical lesions
| Serial no. | Pap smear test
result |
Frequency | % |
| 1 | NILM | 63 | 39.40 |
| 2 | ASCUS | 05 | 3.10 |
| 3 | ASC-H | 05 | 3.10 |
| 4 | LSIL | 40 | 25.00 |
| 5 | HSIL | 17 | 10.60 |
| 6 | Squamous Cell Carcinoma | 30 | 18.75 |
| Total | 160 | 100.00 | |
NILM = Negative for Intraepithelial Lesion or Malignancy, ASCUS = Atypical Squamous cells with Undetermined Significance, LSIL = Lowgrade Squamous Intraepithelial Lesion, HSIL = High grade Squamous Intraepithelial Lesion, ASC-H = Atypical Squamous Cell that cannot exclude HSIL
The histopathological result of 160 cases is presented in Table III. It was revealed that 56 (35.0%) cases had chronic cervicitis, 51 (31.9%) cases mild dysplasia (CIN-I), 14 (8.8%) cases diagnosed as moderate dysplasia (CIN II), 3 (1.9%) patients were severe dysplasia / CIN III and the remaining 36 (22.5%) cases show invasive squamous cell carcinoma (SCC).
Table III: Histological diagnosis of patients with cervical lesions
| SL. no. | Histological
Diagnosis |
Frequency | %
|
| 1 | Chronic Cervicitis | 56 | 35.00 |
| 2 | CIN – I | 51 | 31.90 |
| 3 | CIN II | 14 | 8.80 |
| 4 | CIN III | 3 | 1.90 |
| 5 | Squamous cell carcinoma | 36 | 22.50 |
| Total | 160 | 100 | |
CIN = Cervical Intraepithelial Neoplasia
Table IV shows that on histological examination of 160 cases, a total of 56 (35.00%) cases were found with chronic cervicitis, among them 50 (79.37%) cases were correctly diagnosed previously cytologically as negative for intraepithelial lesion. Out of 51 (31.9%) diagnosed CIN I cases, 34 (85.0%) cases were diagnosed cytologically as LSIL. Out of 14 (8.8%) cases diagnosed as CIN II, 10 (58.82%) cases were diagnosed cytologically HSIL. Out of 3 (1.90%) cases of histologically diagnosed CIN III, 2 (11.76%) cases were diagnosed cytologically as HSIL. The 30 cases were diagnosed cytologically as carcinoma and those cases were histologically confirmed as squamous cell carcinoma. There is highly significant relationship in respect to cytological (PAP smear) and histological diagnoses of cervical lesions in the study group (P<0.005).
Table IV: Comparison of Cytological (PAP smear) and histological diagnoses of cervical lesions
| Frequency in PAP smear diagnosis | Frequency in histological diagnosis | |||||
| Pap smear
Test |
Frequency | Chronic Cervicitis | CIN I | CIN II | CIN III | Squamous cell carcinoma |
| NILM | 63 | 50(79.37) | 13(20.63) | 00 | 00 | 00 |
| ASCUS | 05 | 00 | 3(60.00) | 2(40.00) | 00 | 00 |
| ASCH | 05 | 00 | 00 | 2 (40.00) | 1(20.00) | 2 (40.00) |
| LSIL | 40 | 6 (15.00) | 34 (85.00) | 00 | 00 | 00 |
| HSIL | 17 | 00 | 1 (5.89) | 10 (58.82) | 2 (11.76) | 4 (23.52) |
| Squamous cell carcinoma | 30 | 00 | 00 | 00 | 00 | 30 (100.00) |
| Total | 160 | 56 | 51 | 14 | 03 | 36 |
NILM = Negative for Intraepithelial Lesion or Malignancy, ASCUS = Atypical Squamous cells with Undetermined Significance, LSIL = Lowgrade Squamous Intraepithelial Lesion, HSIL = High grade Squamous Intraepithelial Lesion, ASC-H = Atypical Squamous Cell that cannot exclude HSIL
*Figures within parentheses indicate percentage
The HPV DNA test of cervical lesions was conducted on all 160 cases. The result is shown table V. Out of 160 cases, only 40 (25%) cases were positive and the rest 120 (75%) cases were negative for HPV DNA.
Table V: Diagnosis of cervical Lesions by HPV DNA test (PCR)
| HPV DNA test | Frequency | % |
| Positive | 40 | 25 |
| Negative | 120 | 75 |
| Total | 160 | 100 |
Table VI gives a correspondence result of Histological Diagnosis with Pap smear and HPV DNA test. It was remarkable that out of 36 squamous cell carcinoma cases 31 patients were detected by HPV DNA test. The result further indicates that the cytological diagnosis nearer to the histological findings in almost all cases under this study and in case of high grade lesion and carcinoma it was almost close to positive reaction to HPV DNA test.
Table VI. Correspondence of histological diagnosis with PAP smear and HPV DNA test
| Histological
diagnosis |
Frequency | Frequency of Pap Smear diagnosis | N0. of patients
positive to HPV DNA test |
||||||
| NILM | ASCUS | ASCH | LSIL | HSIL | Squamous cell carcinoma | Positive | Negative | ||
| Chronic
cervicitis |
56 | 50 | – | – | 06 | – | – | 00 | 56 |
| CIN – I | 51 | 33 | 03 | 00 | 34 | 01 | 00 | 02 | 49 |
| CIN – II | 14 | – | 02 | 02 | 10 | – | 05 | 09 | |
| CIN – III | 03 | – | 00 | 01 | 00 | 02 | – | 02 | 01 |
| Squamous cell carcinoma
|
36 | – | – | 02 | – | 04 | 30 | 31 | 05 |
| Total | 160 | 63 | 05 | 05 | 40 | 17 | 30 | 40 | 120 |
NILM = Negative for Intraepithelial Lesion or Malignancy, ASCUS = Atypical Squamous cells with Undetermined Significance, LSIL = Lowgrade Squamous Intraepithelial Lesion, HSIL = High grade Squamous Intraepithelial Lesion, ASC-H = Atypical Squamous Cell that cannot exclude HSIL
The result illustrates that the sensitivity value of this test is almost equal to both Pap test and HPV DNA test, those were found 87.50% and 88.89% respectively. In case of specificity value the Pap test yielded 89.29% and HPV DNA tests yielded higher value, 100%.
Table VII: Comparison of statistical analysis of PAP smear and HPV DNA test
| Statistical value | Pap smear
Cytology in % |
HPV DNA test in % |
| Sensitivity | 87.50 | 88.89 |
| Specificity | 89.29 | 100.00 |
| Accuracy | 88.13 | 96.88 |
| Predictive value of a
positive test |
93.81 | 100.00
|
| Predictive value of a
negative test |
79.37 | 95.83 |
HPV DNA revealed that, HPV – 16 were present in the highest percent (75%), HPV-18 were in 15% and the lowest number of occurrences were HPV – 31 type in 5% and HPV – 52 type in 5 %.
Discussion
The present study focused on traditional Pap smear method and HPV DNA type identification for cervical screening and their comparison with colposcopic biopsy. In this study, 160 VIA positive women were selected. Pap smear cytology, histopathological examination and HPV DNA test were done in every cases. On cytological (Pap Smears) examination it was revealed that 63 (39.4%) cases were diagnosed as Negative for Intraepithelial Lesion or malignancy (NILM), 5 (3.10%) cases were diagnosed as Atypical Squamous Cell of Undetermined Significance (ASCUS) and 5 (3.10%) cases were Atypical Squamous Cell cannot exclude HSIL (ASC- H), 40 (25%) patients with Low Grade Squamous Intraepithelial Lesions (LSIL); 17 (10.6%) patients with high grade squamous intraepithelial lesion (HSIL) and 30 (18.75%) cases were diagnosed as Squamous Cell carcinoma (SCC). A study on patients attending the OPD of BSMMU showed much lower incidence in Pap smear. The percentages of SCC, LSIL and NILM were 0.2%, 4.20% and 91.70% respectively. The lower incidence may be due to incorporation of normal cases in BSMMU study.11
The result of histopathological examinations of 160 cases revealed 56 (35%) cases of chronic cervicitis, 51 (31.9%) cases of mild dysplasia (CIN-I), 14 (8.8%) cases of moderate dysplasia (CIN II), 3 (1.9%) patients of severe dysplasia (CIN III) and the remaining 36(22.5%) cases as invasive squamous cell carcinoma (SCC). Among cytologically diagnosed 30 (18.75%) squamous cell carcinoma cases all were confirmed histologically as squamous cell carcinoma. Highly significant relationship was found with cytological (Pap smear) and histological diagnoses of cervical lesions in this study group (p<0.005).
A study was performed in BSMMU on 70 histologically diagnosed cases of CIN. Out of 70 cases, 34 (48.6%) cases were CIN-I and 36 (50.4%) cases were CIN-II/III.12 Another study from Brazil reported the percentage of CIN-I, CIN-II and squamous cell carcinoma to be 12.0%, 4.3% and 1.0% respectively13. The higher percentage of the present study reflects the inclusion of VIA positive cases only. In Bangladesh a cross sectional study was found and the above occurrences as 21.4%, 10.0% and 29.0% respectively.14
Therefore, out of 160 cases 91(56.88%) cases were correctly diagnosed by cytology, 13 (8.13%) cases were false negative, 6 (3.75%) cases were false positive and 50 (31.25) cases were negative for precancerous and cancerous lesions. There is a significant correlation between Pap smear and Histological findings. Others studies similarly found a significant concordance between Pap smear and histological tests for the diagnosis of precancerous cervical lesions.15,14,16
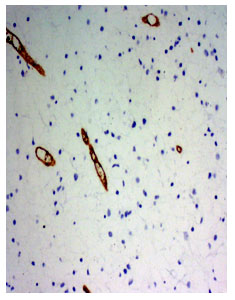
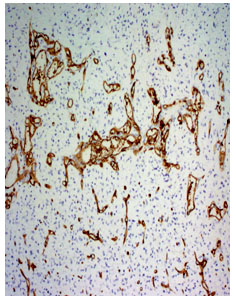
The result of the HPV DNA detection conducted on all 160 cases. Out of 160 cases, only 40 (25.00 %) were found positive and the rest 120 (75.00%) cases were negative. Present study shows that 86.11% positive in cancerous lesions. The technology can find the HPV DNA in almost 100.0% of the invasive cervical cancer cases, 75.00-100.00% of precancerous lesions and 50.00% of borderline lesions’ samples.17,18
.Comparison between HPV DNA test and Pap smear diagnosis represents none of the NILM and ASCUS positive cases exhibited positive reaction to PCR. Among 5(3.10%) ASCH cases 02(40.0%) were PCR positive. Out of 40(25.0%) LSIL cases only 2(5.00%) cases were detected positive. The detection of HSIL cases were found to 11(64.7%) cases out of 17(10.6%) cases. The Squamous cell carcinoma patient’s show out of 30(18.75%) cases 25 (83.33%) cases were positively detected by PCR. The present study indicated that Pap smear cytology is still better than only HPV DNA test for the diagnosis of chronic cervicitis, LSIL, HSIL.
However, a study, comparing the histological diagnosis and it was revealed that none of the chronic cervicitis cases exhibit positive for PCR test.19 Present study also revealed that none of the chronic cervicitis cases show positivity to PCR detection.
The present study has shown that the occurrence of different types of HPV virus be responsible for the causation of cervical cancer. These are detected in samples of patients of cervical lesions. HPV DNA revealed that, HPV – 16 were present in the highest percent (75.00%), HPV-18 were 15.00% and the lowest number of occurrences were HPV – 31 type 5.00 % and HPV – 52 type 5.00 %.
The accuracy of the Pap smears and HPV DNA in this study show to 88.13% and 96.88% respectively. This demonstrates that the accuracy of Pap smears is lower in respect to HPV DNA tests. The accuracy thus determines that the probability of correct diagnosis could be detected by the later tests singly or combined. Specificity in case of Pap smear test is 89.29 and in case case of HPV DNA 100.0%. This means that specificity is higher in DNA test. The sensitivity values of Pap smear cytology and HPV DNA were found 87.5% and 88.89% respectively. The sensitivity value focuses on the ability of a test to correctly diagnose the disease. In this case the cytological diagnostic test is almost equal to DNA test.
Conclusion
It can be concluded that HPV DNA test is not suitable as a single test for detecting precancerous and cancerous lesion than routine Pap smear test. All the cytologically diagnosed NILM (negative for intraepithelial lesion or malignancy) cases and all histologically diagnosed chronic cervicitis cases were HPV DNA test negative. So, mass screening programme does not need HPV DNA test. This will reduce the cost of the screening programme. Combination of cytology (Pap smear) and new technologies such as HPV DNA test would ultimately be more useful. Based on findings, the study recommended that, PAP test should be routinely used in every patient attending the colposcopy clinic, biopsy should be taken in all VIA positive patient and combined pap test and histopathological examination is enough to detect cervical precancerous and cancerous lesion. In our country HPV DNA test is not mandatory as a routine test.
References
- Parkin DM. The global burden of infection-associated cancers in the year 2002. Int. J. Cancer, 2006; 118:3030-44.
- WHO/ICO Information Centre on HPV and Cervical Cancer (HPV Information Centre), 2010. Human Papilloma virus and related cancers in Bangladesh. Summary Report [accessed: 10-03-2013]; available at www.who.int/hpvcentre.
- Carter JR, Ding Z and Rose BR. 2011 HPV infection and cervical disease: A review. Australian and New Zealand Journal of Obstetrics and Gynaecology, 51: 103- 108.
- Tomljenovic L, Shaw CA, Spinosa JP. Human Papillomavirus (HPV), Vaccines as an option for Preventing cervical malignancies; How effective and safe? Current Pharmacological Design, 2013; 19:1-2.
- Crum PC. The Female Genital Tract’ in Robbins and Cotran Pathologic Basis of Diseases. 7th edition Kumar V, Abbas AK and Fausto N (eds) Elsevier Saunders, Philadelphia, 2004; Pp1049-1053.
- Goldie SJ, Kuhn L Denny L, Pollack A, Wright TC. Policy Analysis of Cervical Cancer Screening Strategies in Low-Resource Settings: Clinical Benefits and Cost-effectiveness. JAMA 2001; 285:3107-15.
- ACCP (Alliance for Cervical Cancer Prevention) 2004. Planning and implementing cervical cancer prevention and control programs. A manual for managers. ACCP, Seattle.
- Ngoma T, 2006. World Health Organization cancer priorities in developing countries. Ann. Oncol. 17, Suppl 8, viii9-viii14.
- Sangwa-Lugoma G, Mahmud S, Nasr SH, Liars J, Kayembe PK, Tozin RR, Drouin P, Lorincz A, Ferenczy A, Franco EL. Visual inspection as a cervical cancer screening method in a primary health care setting in Africa. Int. J. Cancer, 2006; 119:1389-95.
- Tahera A, Ashrafunnessa, Jebunnessa R. Development of a visual inspection programme for cervical cancer prevention in Bangladesh. Reproductive Health Matters. 2008; 16(32):78-85.
- Ashrafunnesa, Khatun S, Shamsuddin L, Rahman AJ, Kamal, Kabir S etal. Cervical dysplasia among the women attending gynaecological outpatient department of a teaching hospital. Bangladesh Journal of Medical Science, 2002; 8(1):39-41.
- Ashrafunnesa, Khatun S, Haq F, Islam MN, Hossain MS, Aziz MM et al. 2006.Human Papilloma virus in cervical cancer in Bangladesh. Bangladesh J Obster Gynecol, 2006; 21(2):51-57.
- Syrjänen K, Naud P, Derchain S, Roteli-Martins C, Longatto-Filho A, Tatti S et al. Comparing Pap smear Cytology. Aided Visual Inspection, Screening colposcopy, cervicography and HPV testing as optional screening tools in Latin America. Study design and Baseline Data of the LAMS study. Anticancer research, 2005; 25: 3469-3480.
- Israt T. Study on HPV DNA test and conventional PAP test for identification of cervical intraepithelial lesions and cancer. MD thesis, Dept. of Pathology,2006; Bangabandhu Sheikh Mujib Medical University, Dhaka.
- Islam, Shamina. Relation of Human Papilloma Virus (HPV) load with cervical precancerous and cancerous lesions. MD thesis Department of Pathology,2013; Bangabandhu Sheikh Mujib Medical University, Dhaka.
- Xu Y, Dotto J, Hui Y, Lawton K, Schofield K, and Hui P, 2009. Grade cervical Intraepithelial Neoplasia and Viral load High risk Human Papilloma virus. Significant correlations in patients of 22 years old or younger Int. J. Clin. Exp.Path, 2009; 12:169-175.
- Zhao FH, Lewkowitz AK, Chen F, Lin MJ, HU, SY. Pooled analysis of a Self-sampling HPV DNA test as a Cervical Cancer Primary Screening Method. J. Natl Cancer Inst. 104:1-11 gynecol, 2012; 21(2):51-57.
- Castle PE, Solomon D, Wheeler CM, Gravitt PE, Watchholder S and Schiffman M. 2008. Human pailloma genotype Specificity of Hybrid capture-2 J Clin Microbiol, 2008;46 (8):2595.
- Schiffman M, Wentzensen N. From human papillomavirus to cervical cancer. Obstetrics & Gynecology, 2010; 116(1):177–185.