![]()
Evaluation of Space Occupying Lesion of Liver by Fine Needle Aspiration Cytology and Cell Block Examination
*Sultana SS,1Dewan RK,2 Ferdousi F,3 Sarker R,4 Jinnah SA,5 Jeba R,6 Haque N,7 Hussain M8
To differentiate between benign from malignant tumor and hepatocellular carcinoma from metastatic carcinoma in hepatic space occupying lesion on the basis of cytology and cell block examination this study was done. This was a descriptive cross sectional study comprising of 48 cases, carried out at the department of pathology, Dhaka Medical College during the period of July 2013 to June 2015. Results of all patients were collected and tabulated. Statistical analysis was performed on tabulated data. Out of 48 cases, the cytological diagnosis revealed the highest number of cases of hepatocellular carcinoma 22(45.8%), followed by metastatic carcinoma 13(27.1%), abscess 6(12.5%), hepatocellular dysplasia 3(6.3%) and negative for malignant cell 4(8.3%). Of the total 42 cases of space occupying lesion evaluated by cytology, the diagnoses were similar in cell block, the another six cases contains necrotic debris and cytologically proved as abscess. This measure of agreement is statistically significant with substantial agreement between cell block and cytology status in evaluation of space occupying lesion in liver. Fine needle aspiration cytology in case of space occupying lesion of liver can be relied upon to differentiate between benign and malignant lesion and also primary from secondary lesion. Simultaneous preparation of cell block give no hazard to the patient but provide maximum benefit.
[Journal of Histopathology and Cytopathology, 2018 Jan; 2 (1):11-18]
Key words: Liver, Lesions, cytology, Cell block
- *Dr. Sk Salowa Sultana, Assistant Professor, Department of Pathology, Ad-Din Women’s Medical College, Dhaka. salowasultana257@gmail.com
- Professor Dr. Rezaul Karim Dewan, Professor & Head, Department of Pathology, Dhaka Medical College, Dhaka
- Farjana Ferdousi Lecturer, Department of Cytopathology, National Institute of Cancer Research & Hospital.
- Rabindranath Sarker, Associate Professor, Department of Radiology and Imaging, Dhaka Medical College. Dhaka
- Shahed Ali Jinnah, Associate Professor, Department of Pathology, Dhaka Medical College, Dhaka
- Ruksana Jeba, Associate Professor, Department of Pathology, Dhaka Medical College, Dhaka
- Najmul Haque, Former Associate Professor, Department of Pathology, Dhaka Medical College, Dhaka
- Professor Dr. Maleeha Hussain, Former Professor & Head, Department of Pathology, Dhaka Medical College, Dhaka.
*For correspondence
Introduction
Liver diseases are common health problem throughout the world. Liver diseases are broadly categorized as diffuse and focal lesion. The differential diagnosis of focal lesions are primary liver tumors (benign and malignant), metastatic deposits, congenital and acquired cysts and abscess.1 Appropriate clinical management depends on accurate diagnosis but evaluation of the lesion is a common clinical problem.2 Imaging techniques and serological markers are useful in narrowing the differential diagnosis. Fine needle aspiration cytology (FNAC) mainly indicated in the diagnosis of malignant focal lesions both primary and secondary. FNAC also performed to rule out neoplasm from inflammatory lesion when radiologically inconclusive.3-6
Hepatocellular carcinoma (HCC) is responsible for a large proportion of cancer death worldwide. Also there are demographic variation in the incidence of HCC.7 GLOBOCAN global analysis published moderately high incidence (11-20 per 100,000) in Southeast Asia and also shows 82% of liver cancer cases occurring in developing countries. HCC is preceded by cirrhosis of the liver in most cases. The majority of them are due to viral hepatitis. Indeed, worldwide 50-80% of HCC is due to HBV and (10-25)% of cases are due to HCV infection respectively.8 Dual infection with HBV and HCV is not uncommon in southeast Asia.9 Other causes include alcoholic liver disease, nonalcoholic steatohepatitis, intake of aflatoxin contaminated foods, diabetes and obesity.10
Liver is the most common site of distant metastasis as it filters most of the blood from the body.11 Metastasis commonly arise from tumor of colon, pancreas, breast and lung. Accurate diagnosis of the metastatic lesions is essential in determining the stage of tumor and also for therapeutic and prognostic purposes. The treatment vary from palliative care to partial hepatectomy, specially in those which are potentially chemosensitive or hormonally manipulable. Correlation of clinical, laboratory and radiologic findings is necessary. Radiologically multiple nodules of various sizes distributed randomly suggest metastases5.
The present study was done to evaluate the space occupying lesion of liver by fine needle aspiration cytology accompanying with cell block examination. There are some pitfalls in cytology associated with aspiration of necrotic material and presence of regenerative atypia in hepatocytes. Some of these pitfall can be minimized by using cell block. In cell block, architectural pattern, thickening of cell plate and traversing blood vessels with their lining endothelial cells can be seen. Simultaneous preparation of cellblock from the residual material after smear preparation can help to evaluate the difficult cases.12
Methods
This is a descriptive cross sectional study which was carried out at the department of pathology, Dhaka Medical College, during the period of July, 2013 to June, 2015. The study was done on fine needle aspiration material of liver SOL that were received from Dhaka Medical College and Hospital, and Bangabandhu Sheikh Mujib Medical University (BSMMU).
Patients with radiologically diagnosed SOL in liver and suspected as a case of hepatic neoplasm were included in this study. Patient with bleeding disorders, prolonged prothrombin time, Patient with liver abscess, cyst, haemangioma and already diagnosed cases were excluded from this study.
Relevant clinical informations were recorded. Patients having suspected hepatic neoplasm with good coagulation profile underwent ultrasound guided FNAC. According to standard protocol FNAC was done by an expert pathologist or radiologist and USG guidance was provided by an expert radiologist.
Several cytologic smears were prepared and fixed immediately in 95% alcohol. The smears were left in alcohol at least for 30 minutes at room temperature before staining. The residual material remaining after completion of cytological smears were fixed in 10% formalin and later processed to prepare paraffin embedded blocks .
Smears prepared were stained by papanicolaou stain. Cell blocks were prepared by fixed sediment and bacterial agar method and stained by Hematoxyllin and eosin. Cytopathological examination of the stained slides of hepatic SOL were carried out under light microscope on the same day or next day. Satisfactory smears contained adequate number of representative cells from the target sites. Stained cell block sections were examined to compare the cytological diagnosis.
Results
Table I shows age of the study patients, half of the patients belonged to age 51-70 years. The mean age was found 53.0±15.0 years with range from 18 to 90 years.
It was observed that three fourth (36, 75.0%) patients were male and 12(25.0%) patients were female. Male female ratio was 3:1.
Table II shows cytological diagnosis of the study patients. It was observed that almost half of the patients (45.8%) were found HCC followed by 13(27.1%) were metastasic Ca, 6(12.5%) were abscess and 3(6.3%) were hepatocellular dysplasia .
Table III shows presenting complaints of the study patients. Total 29 patients present with abdominal pain only. Nine patients presented with abdominal lump and pain.
Table IV shows 22 patients were cytologicaliy diagnosed as HCC. Among them 11(50.0%) were HBsAg positive and 2(9.1%) were Anti HCV positive. No case was dual positive. In case of, 42 patients the tumor size was >3 cm, among them 2(66.7%) patients cytologically diagnosed as hepatocellular dysplasia, 22(100.0%) HCC, 13(100.0%) metastatic carcinoma and 5(83.3%) abscess. Total 28 patients presented with multiple SOL. Among them 10 (45.5%) were HCC and 11(84.6%) were metastatic carcinoma.
The association between cell block and cytology status in evaluation of space occupying lesion of liver is given in table VI. Of the total 42 cases of space occupying lesion evaluated by cytology, the diagnosis of 3(75.0%) negative for malignant cell, 2(66.7%) hepatocellular dysplasia, 20(90.9%) HCC and 8(61.5%) metastatic tumour were also similar by cell block. The results of the two methods (cell block and cytology status) analysis found Kappa value = 0.680 with p<0.05. This measure of agreement is statistically significant with substantial agreement between cell block and cytology status in evaluation of space occupying lesion in liver. One of the three cytologically diagnosed hepatocellular dysplasia one was finally proved as HCC after cell block examination.
Table I: Distribution of the study patients by age (n=48)
| Age (years) | Number of patients | Percentage |
| ≤30 | 4 | 8.3 |
| 31-50 | 17 | 35.4 |
| 51-70 | 24 | 50.0 |
| >70 | 3 | 6.3 |
| Mean±SD | 53.0 | ±15.0 |
| Range (min-max) | 18 | -90 |
Table II: Distribution of the study patients by cytology (n=48)
| Cytology | Number of patients | % |
| Negative | 4 | 8.3 |
| HD | 3 | 6.3 |
| HCC | 22 | 45.8 |
| Abscess | 6 | 12.5 |
| MetastasicCa | 13 | 27.1 |
| Adenocarcinoma | 9 | 18.8 |
| Sq. CC | 1 | 2.1 |
| RCC | 1 | 2.1 |
| GIST | 1 | 2.1 |
| Small cell Ca | 1 | 2.1 |
Table I11: Distribution of the study patient with different cytological diagnosis according to clinical feature (n=48)
| Clinical feature | Cytological diagnosis | |||||||||
| Negative
(n=4) |
HD
(n=3) |
HCC
(n=22) |
Metastatic Ca
(n=13) |
Abscess
(n=6)
|
||||||
| n | % | N | % | n | % | n | % | n | % | |
| Abd lump only | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 3 | 23.1 | 0 | 0.0 |
| Abd pain only | 3 | 75.0 | 1 | 33.3 | 15 | 68.2 | 5 | 38.5 | 5 | 83.3 |
| Lump + pain | 0 | 0.0 | 1 | 33.3 | 7 | 31.8 | 1 | 7.7 | 0 | 0.0 |
| Pain + ascitis | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 7.7 | 0 | 0.0 |
Table IV: Distribution of cytologically diagnosed cases with viral marker (n=48)
| Viral marker | Cytologcal diagnosis | |||||||||
| Negative
(n=4) |
HD
(n=3) |
HCC
(n=22) |
MetastasicCa
(n=13) |
Abscess
(n=6) |
||||||
| n | % | n | % | N | % | N | % | n | % | |
| HBsAg | ||||||||||
| Positive | 1 | 25.0 | 0 | 0.0 | 11 | 50.0 | 0 | 0.0 | 0 | 0.0 |
| Negative | 3 | 75.0 | 3 | 100.0 | 11 | 50.0 | 13 | 100.0 | 6 | 100.0 |
| Anti HCV | ||||||||||
| Positive | 0 | 0.0 | 0 | 0.0 | 2 | 9.1 | 0 | 0.0 | 0 | 0.0 |
| Negative | 4 | 100.0 | 3 | 100.0 | 20 | 90.9 | 13 | 100.0 | 6 | 100.0 |
Table V: Association between cytology status with USG finding (n=48)
| USG finding | Cytologycal diagnosis | P value | |||||||||
| Negative
(n=4) |
HD
(n=3) |
HCC
(n=22) |
Metastatic Ca
(n=13) |
Abscess
(n=6) |
|
||||||
| n | % | N | % | n | % | N | % | n | % | ||
| Size | |||||||||||
| ≤3 cm | 4 | 100.0 | 1 | 33.3 | 0 | 0.0 | 0 | 0.0 | 1 | 16.7 | 0.001s |
| >3 cm | 0 | 0.0 | 2 | 66.7 | 22 | 100.0 | 13 | 100.0 | 5 | 83.3 | |
| SOL | |||||||||||
| Single | 1 | 25.0 | 1 | 33.3 | 12 | 54.5 | 2 | 15.4 | 4 | 66.7 | 0.122ns |
| Multiple | 3 | 75.0 | 2 | 66.7 | 10 | 45.5 | 11 | 84.6 | 2 | 33.3 | |
| Diagnosis | |||||||||||
| Primary | 0 | 0.0 | 0 | 0.0 | 13 | 59.1 | 0 | 0.0 | 0 | 0.0 | |
| Secondary | 3 | 75.0 | 2 | 66.7 | 6 | 27.3 | 12 | 92.3 | 0 | 0.0 | 0.001s |
| Not diagnosed | 1 | 25.0 | 1 | 33.3 | 3 | 13.6 | 1 | 7.7 | 6 | 100.0 | |
Table VI: Association between cytological diagnosis with cell block (n=42)
| Cell block | Cytological diagnosis | ||||||||
| Negative
(n=4) |
Hepatocellular dysplasia
(n=3) |
HCC
(n=22) |
Metastatic Tumour
(n=13) |
Inconclusive | |||||
| n | % | N | % | n | % | n | % | ||
| Negative for malignah | 3 | 75.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 |
| Hepatocellular dysplasia | 0 | 0.0 | 2 | 66.7 | 0 | 0.0 | 0 | 0.0 | 0 |
| HCC | 0 | 0.0 | 1 | 33.3 | 20 | 90.9 | 0 | 0.0 | 0 |
| Metastatic tumour | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 8 | 61.5 | 0 |
| Inconclusive | 1 | 25.0 | 0 | 0.0 | 2 | 9.1 | 5 | 38.5 | 0 |
Figure 1. Sex distribution of the study patients
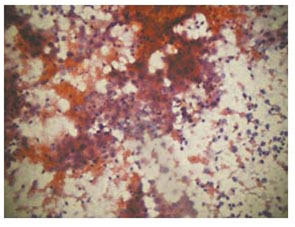
Figure 2. Photomicrograph showing hepatocellular carcinoma (Cytology, Pap stain x40)
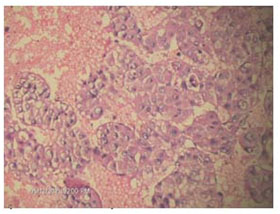
Figure 3. Photomicrograph showing hepatocellular carcinoma (Cell Block, H&E stain x20)

Figure 4. Photomicrograph showing hepatocellular carcinoma (Cell Block, H&E stain x10)
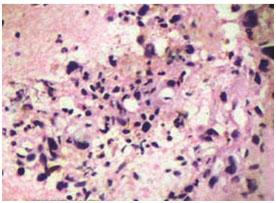
Figure 5. Photomicrograph showing adenocarcinoma (Cell Block, H&E stain x40)
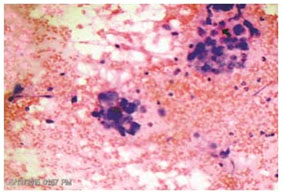
Figure 6. Photomicrograph showing adenocarcinoma (Cytology, H&E stain x20)
Discussion
Liver diseases particularly neoplasia form focal lesion and are often asymptomatic. Even relevant biochemical tests may not show significant changes.13 Diagnosis and management of space occupying lesions in liver is a great challenge. The present study was carried out to evaluate the space occupying lesion of liver by USG guided FNAC.
The mean age of this study cases with hepatic SOL was forth to fifth decades. In Bangladesh Rahman et al (2014)14 showed similar observations. Similar findings were also observed by Nasit et al (2013)3 in India and Nazir et al (2010)4 in Pakistan. In this study, the incidence was more in male than female. According to World Factbook 2014, the finding is similar. In Asia socioeconomic condition and lifestyle favour exposure to hepatitis more in male than female. Risk factors for HBV and HCV infection such as transfusion related spread, sharing of needle and syringes which is common for drug abuser, unprotected sex etc are more prevalent in male.18
Common clinical features were abdominal pain, lump and other constitutional symptom. Most of the patients with HCC presented with only abdominal pain. In metastatic group abdominal pain was frequently accompanied by lump in abdomen. Most of the patients with abscess presented with the complain of abdominal pain. Similar observations regarding the clinical presentations were observed in the study done by Nasit et al (2013)3 and Hossain et al (2010).15
Viral marker was significantly positive in patients with hepatic malignancy. Half of the patients with HCC were HBsAg positive and 9% were anti-HCV positive in this study. Rahman et al (2014)13 and Rahman et al (2010)15 also observed similar findings in Bangladesh.
In present study, most of the cytological diagnosis cases of metastatic carcinoma had multiple SOL in USG. Similar findings regarding distribution of cases according to cytological diagnosis was observed by Mohammed et al (2013)18 and Najir et al (2010). Hepatocellular carcinoma were more than metastatic neoplasm. Also metastatic cases include mostly adenocarcinoma. Similar findings regarding distribution of cases according to cytological diagnosis was observed by Mohammed et al (2013)15 and Najir et al (2010).4 To evaluate the accuracy of USG guided FNAC in hepatic SOL, the cytological diagnosis was compared with cell block. Dysplastic nodules are precursor lesions of HCC and need careful evaluation. In such difficult cases cell block can help in examining architectural pattern as well as ancillary studies. Sometimes cirrhosis, progressing to HCC may have SOL. Cytology of cirrhosis may reveal pleomorphism, multinucleation, stippled cytoplasm and mimic HCC. Cell block in these cases show hepatocytes and bile duct epithelial cells in monolayered sheets. Other pitfall of FNAC related to the diagnosis of well differentiated HCC and poorly differentiated HCC to be distinguished. Architectural pattern, thickening of cell plate, lining and traversing endothelial cell can determine and differentiate in such cases.18 Thus, cell block in addition to smears improve the diagnostic performance and decrease the non diagnostic result.
Conclusion
Treatment modalities are rapidly developing worldwide. Long term survival requires detection of small tumors. The patients with chronic liver diseases and other known primary need regular and proper evaluation. FNAC is a safe, minimum invasive procedure and multiple sample can be obtained with the small diameter needle. FNA cytology in case of SOL of liver can be relied upon to differentiate between benign and malignant lesion and also from primary from secondary. However the indeterminate or inconclusive report is a pitfall , which needs to be minimized. The result can be improved considering with availablity of cell block examination. To get maximum benefit combined approach of FNAC and cell block can be applied.
References
- Leiman G, Liver and Spleen. In: Ovell SR, Stennet GF, Whitaker D, editors. Fine needle aspiration cytology. 3rd New Delhi: Churchil Livingstone; 2003. pp 293-316.
- Swamy M. Arathi CA and Kodardaswamy CR. Value of ultrasonography-guided fine needle aspiration cytology in the investigative sequence of hepatic lesions with an emphasis on hepatocellular carcinoma. J. Cytol, 2011, 28(4): 178-184.
- Nasit J, Patel V, Parikh B, Shah M, Davara K. Fine-needle aspiration cytology & biopsy in hepatic masses: A minimally invasive diagnostic approach. Clin cancer investig J 2013; 2: 132-42.
- Nazir R, Sharif M, Iqbal M and Amin M. Diagnostic Accuracy of Fine Needle Aspiration Cytology in Hepatic Tumors. J of the college of Physicians & surgeons Pakistan 2010; 20(6): 373-376.
- Conrad R, Castelino-Prabhu S, Cobb C, Raza A. Cytopathologic diagnosis of liver Mass lesions. J of Gastrointestinal Oncology, 2013; 4(1): 53-61.
- Asghar F &Riaz S. Diagnostic Accuracy of percutaneous cytodiagnosis of Hepatic Masses by Ultrasound guided Fine Needle Aspiration Cytology. 2010, ANNALS,16:184-188.
- Ng J. Wuu J. Hepatitis B related and Hepatitis C related Hepatocellular Carcinoma in the United States; Similarities and Differences Hepat Mon, 2012, 7635.
- Venook AP, Papandreou C, Furuse J, Guevara L.L.D. The incidence and epitemiology of Hepatocellular carcinoma: A Global and Regional Perspective. The Oncologist, 2010; 15 (Suppl 4):5–13.
- Liu Z, Hou J. Hepatitis B Virus (HBV) and Hepatitis C Virus (Hq) Dual infection. Int J. Med Sci 2006; 3(2):57–62.
- Sanyal AJ, Yoon SK and Lencioni R. The Etiology of Hepatocellular Carcinoma and Consequences for Treatment. The Oncologist, 2010; 15 (suppl 4) 14–22.
- Haque S, Dilawar A and Subzwari J. Ultrasound Guided Fine-Needle Aspiration Biopsy of Metastatic Liver Disease: A Comparative Assessment of Histological & Cytological Techniques. 2012; 28:49-55.
- Nathan N, Narayan E, Smith M and Muuray J Cell Block Cytology: Improved preparation and its Efficacy in Diagnostic Cytology. American Society of Clinical Pathologists, 2000; 114:599-606.
- Evaluation of focal Liver Lesions by Ultrasound as a Prime Imaging Modality. Scholars Journal of Applied Medical Science (SJAMS), 2013; 6(6):1041-1059.
- Rahman F. Role of Cytology .Cell block and Immunohistochemistry in Differentiating Hepatocellular Carcinoma from MetastaticTumors in Liver.Unpublished MD thesis, 2014; BSMMU, Bangladesh.
- Hossain M. Characterization of Focal liver mass by computed Tomography scan with Cytopathological Correlation. Unpublished MD thesis, 2010; BSMMU, Bangladesh.
- Rahman AA. Prevalence of Primary HCC &Secondaries in liver in it attending Dept of Gastr&Hepatology in BSMMU. Unpublished MD thesis,2010; BSMMU, Bangladesh.
- Charles E, Ray MD, William S, Rilong MD (2006) Current Imaging Strategies of primary & Secondary Neoplasm of the liver. Sem: Int: Rad: Mar: 2006; 23(1):3-12.
- Mohammed AA Elsiddig S, Abdul Hamid M, Gasim G and Adam I. Ultrasound guided fine needle aspiration cytology and cell block in the diagnosis of focal liver lesions at Khartoum Hospital, Sudan. 2012;7:
- Barbhaiya M. Bhunia S, Kakka M, et al. Fine Needle Aspiration Cytology of lesions of liver and gallbladder: An analysis of 400 consecutive aspirations. J Cytol, 2014; 31(1): 20-24.