The Incidental Findings of Thyroid Neoplasms in 200 Sequential Autopsies in Dhaka Medical College
*Awal N,1 Dewan RK,2 Ray S,3 Ferdous JN4
- *Dr. Naila Awal, Assistant Professor, Department of Pathology, Greenlife Medical College. nailaawal@gmail.com
- Rezaul Karim Dewan, Professor and Head, Department of Pathology, Dhaka Medical College.
- Subrata Ray, Assistant Professor, Department of Pathology, Jessore Medical College.
- Jesmin Naz Ferdous, Assistant Professor, Department of Pathology, Sir Salimullah Medical College.
*For correspondence
Abstract
Background: The incidental findings may contribute to identify many common latent thyroid neoplasms. The study was carried out to evaluate the frequency of undiagnosed thyroid neoplasms existing in the general population of our country.
Methods: Total 200 whole thyroid glands were collected from the deceased who had apparently normal thyroid gland. The study includes 85 male and 115 female cadavers between 14 to 65 years of age. Sections were taken from grossly identified lesions for histopathological process, and studied microscopically, other areas were collected randomly for microscopic examination.
Result: In all cases, both benign and malignant neoplasms were incidental findings, seen in 4.5% of the cases. Malignant neoplasm was found in 2% of cases and was latent.
Conclusion: Clinically normal appearing thyroid glands may contain major pathological lesions, when they are microscopically studied. Considering the high prevalence of thyroid malignancy to other parts of the world, routine systematic examination of the gland is recommended to detect unsuspected thyroid pathology mainly carcinoma.
[Journal of Histopathology and Cytopathology, 2019 Jul; 3 (2):93-98]
Key words: Occult neoplasm, thyroid
Introduction
Thyroid cancer is the fifth most common cancer in women worldwide.1 In most countries, incidence have been appreciably increasing over the last few decades.2,3 If recent trend is maintained, thyroid cancer may become the fourth most common cancer by 2030 in United States.4
Small “occult” thyroid carcinomas are present in a substantial proportion of the general population. In surgical practice, biopsy of thyroid without symptom is not indicated. So, autopsy sample can be an alternative to assess the incidence of latent thyroid neoplasms.
Usually, the thyroid gland is not examined in routine autopsies in Dhaka Medical College. When a more careful and systematic study of the thyroid is done in autopsy material, latent thyroid lesions are found in a frequency of 20 times greater than the incidence seen at routine autopsy series (0.8 %).5 Pingitore R, (1982) found 3.6 % of latent carcinomas in his autopsy specimen.6 There is no data of unsuspected thyroid neoplasm after a systematic and histologic examination of the gland during autopsy in Bangladesh.
The present study was designed to determine the frequency and evaluation of the prevalence of incidental carcinomas in our population in autopsy specimen. It may be of interest in regard to causal or prognostic factors.
Methods
This study was initiated after receiving approval of the ethical committee of our institution. It is cross-sectional descriptive study with convenient sampling done over a period of two years (January 2016 to December 2017). The study population comprised deceased undergoing medicolegal autopsy in morgue under the Forensic Medicine Department of Dhaka Medical College. The specimen was discarded if obtained from decomposed or mutilated body or when there was injury over the neck involving thyroid gland as well as from the subject in whom there was previous hemi thyroidectomy. Enlarged thyroid beyond normal range was also discarded from this study.
After receiving the specimen, it was fixed in 10% neutral buffered formalin and dissected free from surrounding neck tissues. The thyroid glands were weighed, measured and divided into right and left lobes with isthmus attached to one of lobes.
The whole thyroid gland was divided into three parts and labeled as anterior, middle and posterior from superior pole to inferior pole. The lobes were serially sectioned at 2 mm intervals from 16 areas of both lobes and isthmus.
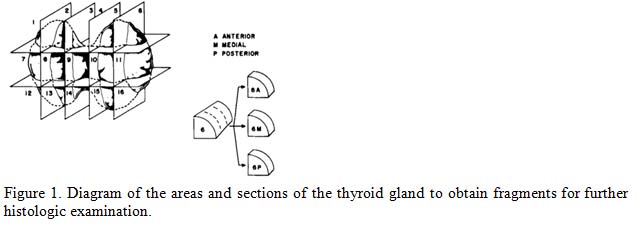
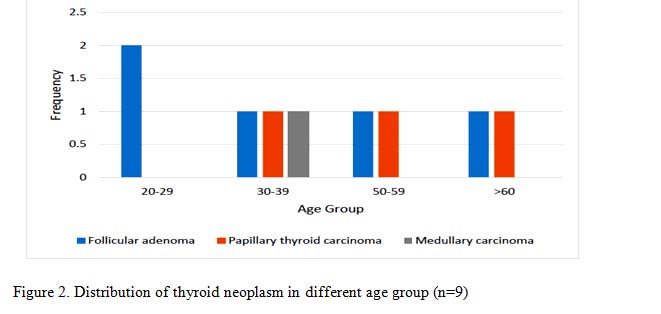
Figure 1. Diagram of the areas and sections of the thyroid gland to obtain fragments for further histologic examination.
All grossly visible lesions were noted and many were photographed. Histological sections were made from all grossly visible lesions. If no gross lesions was identified at least one histologic section was prepared from each lobe of the glands and were processed. All the sections were stained with hematoxylin and eosin. The prepared slides were examined and the findings were noted. Special stain was donein selected cases.
Data was collected, compiled and properly tabulated in master chart. Representative tables and graphs were made and subjected to suitable statistical analysis by using appropriate methods.
Result
Among 200 cases, 85 cases (42.5%) were male and 115 cases (57.5%) were female. The male female ratio was 1: 1.36. The age of the study subject was 14 to 65 years with mean age 24.48± 12.09 years. The mean weight of thyroid gland was 15.50 ± 4.43 gm.
Neoplasm was seen in 9 cases out of 200 cases (4%). The youngest cadaver was 25 years and the oldest was 65 years of age. Major incidence occurred in 3rd decade. The most common neoplasm was follicular adenoma (5 cases, 2.5 %) followed by malignant neoplasm (4 cases, 2 %). The malignant neoplasm was papillary thyroid carcinoma and medullary thyroid carcinoma (1 case, 0.5%). All neoplasm was restricted to single lobe of thyroid except in one papillary thyroid carcinoma, where tumor foci were multiple involving left lobe and isthmus of thyroid
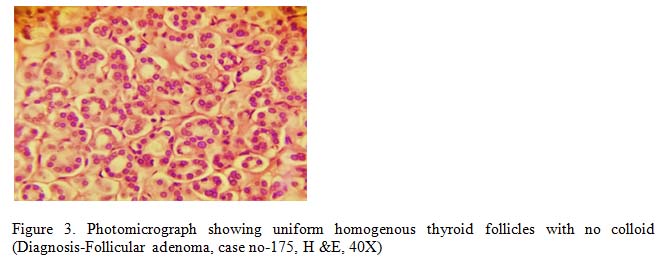
Follicular adenoma was the most common benign neoplastic lesion of solitary thyroid nodule. A total of 5 cases (3%) was diagnosed histologically as follicular adenoma, 3 cases were male and 2 cases were female. The size of the adenoma varied from 0.2 to 1.1 cm in diameter and had single foci distributed in single lobe of thyroid. Microscopically, they showed well demarcated areas consisting of numerous small uniform follicles with scanty colloid. The neoplastic cell showed follicular morphology. No capsular and vascular invasion was identified in any of the cases.
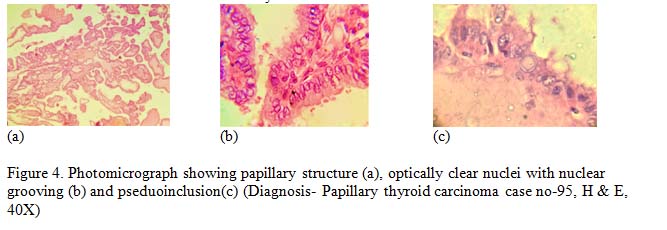
Among the malignant neoplasm, 3 cases (1.5%) were revealed as latent papillary thyroid carcinoma based on characteristic nuclear feature. None was encapsulated. All of these lesions were within 1 cm in maximum diameter. By definition, the tumors were diagnosed as papillary microcarcinoma.7 One of them was follicular variant of papillary carcinoma presented with ground glass appearance of nucleus and formation of follicles. Some of the neoplastic cells showed intranuclear groove. Psammoma bodies were not found in any cases.
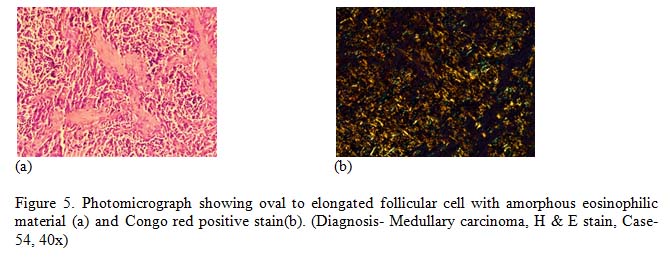
The only one case diagnosed as medullary carcinoma, composed of polygonal to spindle shaped cells forming nests. Acellular amorphous amyloid deposition was seen in stroma. Special stain Congo red was done and supported the diagnosis by green birefringence of amyloid.
Discussion
The incidental findings can contribute to discover many common thyroid lesions. The incidence of both benign and malignant lesions of thyroid varies widely in different geographical areas in the world.
This study was carried out with a view to evaluate the frequency of undiagnosed thyroid neoplasms existing in the general population of our country.
The incidence of thyroid carcinoma differs in different countries range from 0.5 to 10 per 105 persons.8 In most countries, papillary carcinoma was the most common histologic type, comprising approximately 40-70 % of all thyroid malignancy.8
In our study, the weight of thyroid gland with latent neoplasm (17.66 ± 4.03 gm) was similar to that of glands without neoplasm(15.39 ± 4.43 gm), because of we include apparently normal thyroid gland with normal weight. This correlates with previous study done by Ottino et al, (1989).9
The most common thyroid neoplasm of this study was follicular adenoma (3%, 5 cases) which is similar to the study done by Bisi, et al. (1989) which was 4.33%.10 Among the malignant neoplasms, one was medullary carcinoma and rest of three were papillary microcarcinoma. Papillary thyroid microcarcinoma is a specific subgroup of papillary thyroid carcinoma and defined by WHO on the largest dimension of 1.0 cm or less.7,11 Most of Papillary thyroid microcarcinoma are not detectable in clinical examination and are diagnosed incidentally during pathologic examination of thyroid specimens after surgery for benign thyroid diseases or in autopsies.11
The rate of malignancy in this study was 2% (4 cases) whereas in a previous study done by das et al, (2017) the rate of malignancy was 2.1% (5 out of 240 cases) which is similar to our study.12 On the other hand, study done by Bondenson and Ljungberg (1981), they estimated rate of malignancy was 8.6 %.13 The higher prevalence of their study was probably due to large number of study subject. The study done by Furmanchuk and Rusak (1992), the estimated rate of malignancy was 9.9% (11 out of 122).14 The higher prevalence of their study was probably due to radiation and other hazard.14 Following tables show the prevalence rate (%) of occult papillary carcinoma in different autopsy series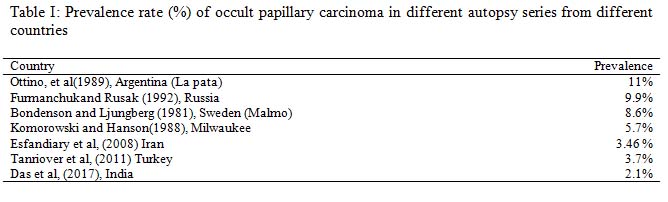
Conclusion
Many thyroid neoplasms may remain silent and diagnosed only autopsy during histopathological examination of specimen. So routine systematic examination of the gland is recommended to detect unsuspected thyroid neoplasm mainly carcinoma.
The presence of 2 % (4 cases out of 200) of malignant thyroid neoplasm in this study speaks about the burden of this disease in our population which may be detected by thorough thyroid screening test.
The latent thyroid diseases including thyroid carcinoma is treatable and have good prognosis. So, routine evaluation of thyroid status by thyroid function tests in a reasonable time interval can be done to evaluate the latent thyroid neoplasm. Routine systematic examination of thyroid gland during autopsy not only would be useful in determining the cause of death but also contribute to the social health data by yielding the frequency of latent thyroid neoplasm.
References
- Jemal A, Siegel R and Ward E. Cancer statistics 2010. A Cancer Journal for clinicians 2010; 60(5):277-300.
- Davies L, Welch HG. Increasing incidence of thyroid cancer in United States, 1973-2002, JAMA, 2006;295(18):2164-7.
- Horn-Ross PL, Lichtensztajn DY, Clarke CA, Dosiou C, Oakley-Girvan I, Reynolds P et al. Continued rapid increase in thyroid cancer incidence in California: trends by patient, tumor and neighborhood characteristics. Cancer Epidemitol Biomakersprev 2014; 23:1067-79.
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver and pancreas cancers in the United States. Cancer Res 2014;74(11):2913-21.
- Silverberg SG and Vidone RA. Carcinoma of the thyroid in surgical and post-mortem material: Analysis of 300 cases at autopsy and literature review. Ann Surg 1966;164:291-299.
- Pingitore RR. Morfologiciautopticisu 111 tiroidiclinicamentenormali in un’ are aitalianasenzaedemiagozzigena. Purhologica 1982;14:545-552.
- Rosai J (2004). Rosai and Ackerman’s Surgical Pathology. 10th ed. St. Luis: Mosby.
- Harach HR, Franssila KO, Wasenius V. Occult Papillary Carcinoma of the Thyroid. A “Normal” Finding in Finland. A systematic Autopsy Study. Cancer, 1984; 108:529-530.
- Ottino A, Pianzola HM, Castelletto RH. Occult papillary thyroid carcinoma at autopsy in La Plata, Argentina. Cancer 1989;64:949-50.
- Bisi H, Fernandes VS, de Camargo RY, Koch L, Abdo AH, de Brito T. The Prevalence of Unsuspected Thyroid Pathology in 300 Sequential Autopsies, With Special Reference to the Incidental Carcinoma. Cancer 1989; 64:1888-1893.
- Dideban S, Abdollahi A, Meysamie A, Sedghi S, Shahriari M. Thyroid Papillary microcarcinoma: Etiology, clinical manifestations, Diagnosis, Follow-up, Histopathology and Prognosis. Iran J Pathol, 2016:11(1):1-19.
- Das MM, Jain BB, Sukul B, Chattopadhyay S. A histopathological study of autopsied thyroid. Thyroid Res Pract, 2017:14 (3):112-117.
- Bondenson L, Ljungberg O. Occult thyroid carcinoma at autopsy in Malmo, Sweden. Cancer, 1981;47:319-323.
- Furmanchuk AV, Rusak NI,(1992). Latent cancerous pathology of the thyroid. Vopr Onkol, 1992;38(7):811-7.